|
ERYTHEMAS AND URTICARIA
|
|
|
|
Erythema means redness of the skin due to dilatation of blood vessels. This will lead to hyperemia in a specific area of the skin in response to endogenous or exogenous factors. Erythema is the first and most common skin manifestation, which may be localized or generalized. Different clinical types of erythema
TOXIC
ERYTHEMA OF THE NEWBORN Erythema toxicum neonatorum is a patchy benign eruption of the newborn that appears in the first three or four days of life and generally disappears by the second week. Etiology The cause of this type of erythema of the newborn is unknown. Different factors are suspected: An allergic origin : hypersensitivity to milk. Drugs transmitted to the infant via the placenta .
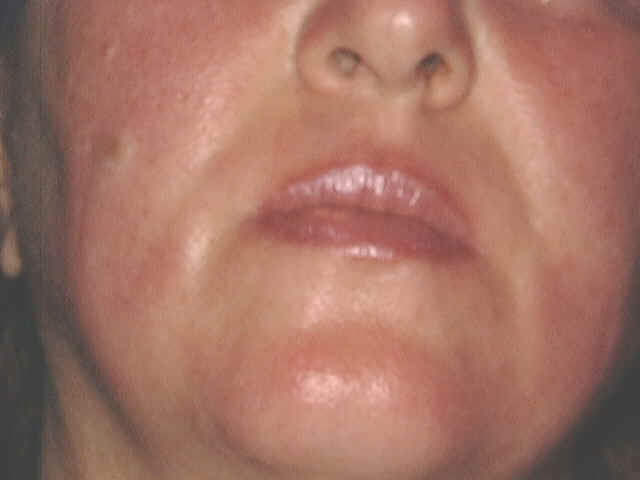
Fig.220d. Erythema due to drug reaction(Corticosteroids) Due to vaginal secretions of the mother. Allergic response to some components of sebum . Clinical Features Skin lesions initially appear as erythematous blotchy macules, papules or pustules mainly on the trunk , face and proximal parts of the limbs. Rarely the palms and soles are affected. The papules may be surmounted by small pustules, 2-4 mm in diameter. In the mildest cases these macules fade within a day. In more severe cases, urticarial papules arise within the erythematous areas, on the back and buttocks. The general health of the infant is not affected and usually the lesions fade away without treatment . Differential Diagnosis Toxic erythema of the newborn has to be differentiated from: Pustular miliaria, which clinically simulates toxic erythema. Herpes simplex virus infection . Incontinentia pigmenti . Neonatal pustular pyoderma : The pustules show neutrophilic leukocytes.The pustules in erythema neonatorum toxicum are filled with eosinophils which are follicular and perifollicular . The erythematous macules show slight perivascular infiltration with eosinophils. Treatment Symptomatic and supportive measures since no specific treatment is available. Usually the skin lesion clears within few days .
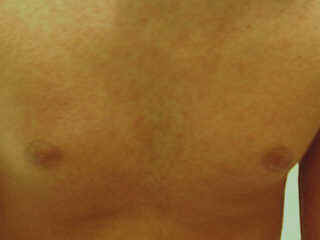
Several types of exanthematous diseases manifest with erythema, which is variable and specific to such diseases. Viral and bacterial diseases are common cause of erythema in infants and children. Measles, erythema infectiosum (fifth disease), roseola and scarlet fever are some types of generalized erythema.
Fig. 220d,e, Generalized exanthematous reaction
ERYTHEMA
INFECTIOSUM Epidemic types of generalized erythema were reported in Holland and Germany in 1958 in children, known as "Margarine disease" . Viral cause from certain types of diary products was suspected. The disease is slightly infectious that occurs in epidemics in spring and summer. Clinical features The erythema appears on the proximal parts of the extremities and sometimes on the face and spread to cover the entire skin surface.Erythema appears suddenly and usually without any prodromal symptoms. The erythematous reaction has different clinical features simulating erythema multiforme,papular and morbiliform eruption. The skin lesion on the face has the butterfly appearance and present with diffuse erythema or grouped tiny papules on an erythematous base. Itching is severe but on the fifth day , erythema begins to regress and itching becomes less.
ERYTHEMA
MULTIFORME This is a hypersensitivity syndrome due to antigen-antibody reaction, which may involve skin, mucous membranes and internal organs. Stevens and Johnson‘s syndrome is an acute and severe clinical type of erythema multiforme.
Clinical Features Skin lesions present with symmetrical bright bluish to dark purple slightly infiltrated, round macules with tendency to spread peripherally. Different clinical types of erythema multiforme may appear, which depend mainly on the shape and severity of the reaction. Skin lesions may be macular,papular,nodular, vesicular or bullous forming different shapes such as the annular, circinate, the iris lesions, purpuric and urticarial types. The Iris lesion: The central portion of the lesion usually shows a bluish gray central depression known as the “iris lesions“ which is usually characteristic to erythema multiforme.
The most common sites involved are the dorsal aspects of the hands, fingers and feet. The Hebra type: is characterized by symmetrical erythematous papular, urticarial, bullous or even hemorrhagic reactions appear on the sun-exposed areas of the skin. Skin lesions have the characteristic iris lesions. The mucous membranes are usually involved. This type is usually recurrent and usually preceded by herpes labilalis before the onset of erythema. The maculopapular type Well-defined erythematous maculopapules, which spread peripherally forming polycyclic patches with central clearing. Erythema iris may be conspicuous.
Fig. 223b. Maculopapular erythema The bullous type Skin lesions may show hemorrhagic bullae on an erythematous base. The vesiculobullous type Discrete or grouped vesicles surrounded by an erythematous base, which may be misdiagnosed as herpes lesions. The maculopapular type Skin lesions present with edematous bright bluish red macules or flat-topped papules, which has the tendency to spread peripherally.
This is considered as a severe type of erythema multiforme which presents with skin , mucous membrane and internal manifestations. General manifestations The patient may show severe constitutional manifestations, where the severity and prognosis depend on age, cause of the disease and early management. Constitutional symptoms : fever, headache, malaise and soreness of the mouth and throat. The syndrome may present with severe manifestations such as rapid pulse,weakness,rapid respiration, prostration and joint pains. The syndrome may be fatal. Mucous membrane : stomatitis is the early manifestation and may be diagnostic. Mucous membranes show ulceration with bleeding, salivation and angioedema.This may interfere with drinking or feeding causing more cachexia to the patients.Conjunctivitis, corneal ulceration,rhinitis and epistaxis are common mucous membrane manifestations.
Fig. 224a.
Steven’s Johnson syndrome
Fig. 224b.Steven’s Johnson syndrome
Fig. 224c.Steven’s Johnson syndrome (Vesiculo-bullous lesions)
Skin manifestations: skin lesions present with multiforme, erythematous, macular with an iris,papular,vesicular reaction with large hemorrhagic bullae on an erythematous base. Rupture of the bullae lead to ulcerating abraded skin surface, which is susceptible to secondary infections. Subungual hemorrhages are common. Purpura is a common manifestation of the severe type. Pruritus may be severe. Etiology Different factors are blamed as a causative of Steven-Johnson syndrome. Idiopathic types with unknown cause are common. Some of the following may cause the syndrome:
Histopathology Inflammatory infiltrate of the upper dermis. Spongiosis and edema of the epidermis and dermis. Perivascular inflammatory infiltrate around dilated blood vessels. Extravasated erythrocytes. Differential diagnosis Toxic epidermal necrolysis. Bullous contact dermatitis. Pemphigus and pemphigoides. Bullous systemic lupus erythematosus. Treatment Treatment depends on the cause and the severity of the clinical manifestations.
Erythema elevatum diutinum is characterized by slightly painful, red,elevated, round, polygonal nodules, usually arranged in annular shapes. The most common sites involved are the extensor surfaces of the extremities and hands.
Fig.224e. Erythema Elevatum diutenum
The nodules have smooth surface showing central depression. The eruption has a chronic course, which may extend for months.There is no involvement of the mucous membranes and the general health is no affected.
Erythema nodosum is characterized by symmetrical , tender, bright red nodules of different sizes, most common on the extensor surfaces of the legs. Mild constitutional symptoms such as fever,malais,myalgia and arthralgia may precede the appearance of the eruption.The disease is self-limiting.
Fig.224f. Erythema nodosum (Erythema nodosum was discussed in the previous chapters).
This type is common in children with rheumatic fever and rheumatic endocarditis. Skin manifestations present with pale red to livid rings of variable sizes and shapes. The commonest sites involved are thighs,abdomen, chest and the back.
The disease runs a chronic course, and may begin at any age even in newborn infants . In neonates, annular erythema may be a sign of maternal systemic lupus erythematosus. The most common sites are the buttocks, thighs and upper arms, but any area may be involved. Sometimes lesions are localized on the extremities but the face is seldom affected.
Clinical Manifestations The lesions may be solitary or more often multiple that appear mainly on the buttocks , thighs and upper arms. Small, pink, infiltrated papule slowly enlarges and forms a ring as the central area flattens and fades. Individual lesions last for a few days, weeks, or slowly extend for months, with the appearance of purpura and pigmentation . Extension of the lesion may be irregular to leave arciform segments. The edge may be quite flat or easily palpable, smooth or show slight scaling. Rarely vesiculation occurs. Itching is variable but seldom intense.
Erythroderma means erythema and skin scaling . Erythroderma may be primary or secondary that occurs in the course of different skin diseases . Primary erythroderma Erythroderma desquamativum (Linear‘s disease). Erythroderma associated with lymphomas, Hodgkin‘s disease, and mycosis fungoides.
Metabolic complications of erythroderma Hyperthermia: sweat retention due to obstruction of sweat gland orifices may lead to dangerous hypothermia especially in children in the tropics . Muscle wasting: An increase in metabolic activity provides compensatory increase in body heat production but at the expense of tissue catabolism Cardiovascular failure: Skin blood flow, blood volume and cardiac output may all be increased. If these changes persist, they may lead to cardiovascular failure. Malabsorption and enteropathy may occur. Hypoalbuminaemia: Extensive scaling leads to protein and iron loss beside impaired absorption and utilization, causing edema and iron deficiency anemia . Serum B12 tend to be low, mainly due to increased utilization by the hyperplastic epidermis. Dehydration and water loss: The barrier efficiency of the skin in psoriatic erythroderma is certainly impaired. The chief effect is the increase in water loss by diffusion since evaporation of which also contributes to heat loss. The urine output tends to drop and if water intake is inadequate for any reason, dehydration results. Diagnosis: Erythroderma may be suspected in an infant with erythroderma that has persisted from birth or shortly after birth. Failure to thrive and diarrhea. Susceptibility to infections. Lymphadenopathy, and/or hepatospleenomegaly will help to establish the diagnosis. Differential Diagnosis Non-bullous ichthyosiform erythroderma . Omenn‘s syndrome . Erythrodermic atopic eczema . Psoriasis .
Urticaria is a common vascular skin reaction characterized by the appearance of wheals that are transient and recurrent. These are erythematous, elevated skin swelling surrounded by a halo and accompanied by severe itching or stinging sensation. Urticaria may be accompanied by systemic manifestations such as asthma, abdominal cramps, joint pain and severe laryngeal edema . Urticaria is common in children and has different clinical picture that may appear with different shapes , and varies from the simple wheal to the severe bullous type .
Urticaria(Drug reaction ,Amoxycillin)
Fig.227 Urticaria Neonatal hemorrhagic edema (purpura en cocarde) occurs in very young children and is on the borderline between urticaria and vasculitis. Urticarial lesions show vascular dilatation. The reaction in urticaria is related to different factors; histamine (mediator for the common urticaria), kinins (mediator for angioedema), serotenin , prostaglandin, anaphphylatoxin and acetylcholine release . The different factors affecting children are the same as that of adults with a tendency to be more acute in young ages . Classification of Urticaria Urticaria is classified according to its etiology into immunological or non-immunological type .
Diagnosis Patient presenting with chronic urticaria should be thoroughly investigated. This doesn‘t mean to do immediately every possible investigation to diagnose or exclude every possible underlying cause . History and a careful interrogation of the patient or the child‘s mother may be very helpful to reach the diagnosis of the triggering factors. Food: The relation to food especially food with additives, colored or preserved foods should be considered . Drugs: taken by the child such as antibiotics or antipyretics as salicylates should be thoroughly investigated. Systemic Diseases: Urticaria may appear with other diseases such as systemic diseases or hormonal imbalance. Insects: ants , mosquitoes may cause severe reaction especially in sensitive infants .
The psychological state of the child is important where some cases of urticaria are due to stress and psychological trauma . Investigations Investigations of chronic recurrent urticaria is not always successful in detecting the offending causative factors . Several tests may be considered such as:
There are different types of urticaria : Cholenergic urticaria Physical urticaria . Herido-familial urticaria Idiopathic urticaria . Angio neurotic edema Urticaria pigmentosa Papular urticaria Bullous urticaria Inhalant urticaria Physical agents such as cold, heat and sun may precipitate this type of urticaria. Cold urticaria Cold urticaria may be transmitted as an autosomal dominant . The skin lesions present with wheals that appear after exposure to cold . The condition begins after birth and may persist throughout life . Another type of cold urticaria accompanies collagen diseases such as lupus erythematosus, dysproteinaemia or haemoglobinuria. Idiopathic cold urticaria This is a common type of urticaria, where whealing appears after exposure to cold and can be relieved after warming of the skin . Mucous membrane of the mouth , pharynx and gastrointestinal tract may be involved. Patients having this type of urticaria should have much care and should be warned not to be exposed suddenly to cold or swimming in cold water or having a cold shower, where these may cause syncope and even sudden death. Diagnosis of cold urticaria is by applying an ice on the skin, this will provoke an urticarial lesion . Heat urticaria Urticarial lesions appear due to histamine release after sweating initiated by heat or after bathing with hot water . Solar urticaria Urticarial lesion appears few minuets after exposure to sunlight . This condition may be associated with the delayed type of photosensitivity and polymorphous light eruption .
Demographic urticaria is a common type, characterized by linear and with sharp edged wheals, appearing after scratching of the skin by a blunt object. This is associated with increase in the circulating IgE.
Clinical Features This type of urticaria can be provoked by pressure of tight clothes or after stroking the skin, where few seconds later a wheal with a surrounding erythematous flare corresponds to the affected sites. This may be accompanied by itching . Scratching also leads to the appearance of linear raised erythematous streaks . Treatment of urticaria Suspected food and drugs should be eliminated . Hydroxyzine (Atarax) is considered specific in the treatment of such type of urticaria . The new generation antihistamine; Cetrizine (Zyrtec) is also of value. Topical steroids are not always recommended . Oral and parental steroids are temporarily effective and rarely indicated in infants and children . H2 blockers such as Cimetidine may be tried in chronic and resistant cases . Cyproheptadine (Periactin): May be given to older children and not to young age. This drug may be effective especially if combined with hydroxazine. Sometimes a combination of two antihistamines of the different group may be necessary in older children . Tricyclic antidepressants, such as doxepin, have the capability to block both H1 and H2 receptors. Leukotriene receptor antagonists and oral beta-adrenergic agents are reported to be helpful as combination therapy with antihistamines. Low-dose thyroid hormone for patients who have positive antithyroid antibodies . Cyclosporin, hydroxychloroquine, colchicine, dapsone, and COX 2 inhibitors have also been used in some cases not responding to traditional treatment. This type of urticaria is herido-familial dominantly transmitted due to absence of C1 esterase inhibitor, which normally inhibits the activity of the first component of the complement . Clinical Manifestations The manifestations begin early in childhood and are characterized by recurrent attacks of swelling of the subcutaneous tissue, lips, mouth and eyes. The condition may be precipitated by injury where non-itchy, firm and painful lesions appear. Constitutional symptoms: severe abdominal colic due to gastro-intestinal tract involvement may be a manifestation in some cases . Respiratory tract :may be involved and in severe cases it may cause asphyxia in infants and children . Diagnosis Diagnosis of herido-familial urticaria depends on : Absence of typical urticarial lesions . Severe angioedema . Tender subcutaneous tissue . Respiratory symptoms . Abdominal colic due to gastro-intestinal involvement . Decreased of C1 esterase inhibitor,C2 and C4 complement components. Treatment Treatment is sometimes disappointing in such cases, where the mortality rate is considered high . Fresh plasma replacement of esterase inhibitor may have some effect . Epsilon-aminocaproic acid and Danazol ( weak androgen which inhibits pituitary gonadotrophin ) both proved to be effective prophylactic medications.
Urticaria pigmentosa is an uncommon dermatoses that usually develops during the first year of life . The condition is characterized by urticarial lesions due to histamine release from excess mast cells in the skin and may be associated with systemic manifestations. Types of Urticaria Pigmentosa
N.B. The patients should be warned not to rub the body vigorously especially during and after bathing with hot water, where this may activate mast cells in the skin and respiratory tract which may lead to flushing , hypotension, bronchospasm and even sudden death . Treatment Antihistamine H1 blockers and cyproheptadine may give some relief . H2 blockers claimed to have some effect in alleviating symptoms in urticaria pigmentosa . Systemic manifestations can be treated accordingly .
|









































| Contents | << Previous Chapter | Next Chapter >> | Search |