|
DISEASES OF SEBACEOUS GLAND ACNE
|
|
|
|
Acne is rare in children and old age. The sites involved are the seborrheic areas rich in sebaceous glands mainly face, upper chest , back and the shoulder areas. The usual types of acne occur after puberty. Since puberty manifests earlier nowadays in some children especially young girls, brief discussion of different types of acne are included in this chapter. Etiology Increase in the activity of sebaceous glands and occlusion of the pilosebaceous orifices are the main factors of acne pathogenesis. Hormones : Androgens increase the activity of sebaceous gland in both sexes. Estrogens antagonize the effect of androgens. ACTH increases the activity of the sebaceous glands due to its stimulation of production androgens. Infections: Corynebacterium acnes and staphylococci are considered important in the pathogenesis of acne. Diet: The effect of diet is variable. Some types of diet such as high carbohydrate, fatty foodstuffs, chocolate, diets rich in iodides such as seafood may have some effect on exacerbation and not the pathogenesis of acne in certain individuals. Drugs: acniform eruption results due to different systemic and topical medications. Tetracyclines , corticosteroids, certain vitamins with mineral supplements such as iodides and other drugs may be accompanied by acniform eruptions. Stress and lack of sleep may have some role. Pathogenesis Two factors play an important role in the formation of acne. These include increased activity of sebaceous glands with production of excess sebum and the other is the occlusion of the pilo sebaceous orifices.
( A)
(B)
(C) Hormones :
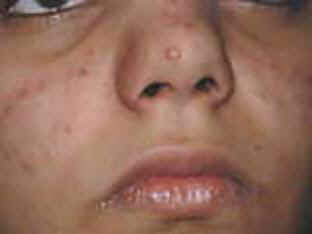
Fig. Acne vulgaris : (Black heads &papulopustules) Increased activity of sebaceous glands and occlusion of the cornfied hypertrophic pilosebaceous follicles lead to retention of sebum into the follicles, which dilate and rupture by time. Anaerobes such as Corynebacterium acne, Pityrosporon ovale and Staphylococci cause split of the sebum into fatty acids and triglycerides which act as an important irritating factors .This will lead to the formation of the different clinical types of acne which varies from papules, pustules ,cysts and comedones.
Skin lesion begins shortly after birth as small papules on the seborrheic areas mainly on the forehead and cheeks due to increase in the activity of sebaceous glands. The role of circulating androgen and estrogen may have some role. There is usually a family history of severe acne . The condition resolves spontaneously within few weeks . Persistent cases may need antiseptic lotions such as Clindamycin or Erythrocin topically .
This type of acne affects mainly males, presents as facial acne at around three months and may last up to five years of age . Etiology
Topical preparations: erythromycin (Eryderm) or Clinamycin lotion (Dalacin). Pufexamac (Parfenac or Flogocid cream) may have good effect especially when there is erythema or irritations of lesions by previous medications. Benzoyl peroxide or vitamin A acid is useful medications .These preparations are better used for adults since they may cause irritation in some patients especially when applied to extensive areas.
Cysts containing thick , viscid or blood tinged fluid . The most common sites involved are the face and the back. This type has to be differentiated from the cysts of neurofibromatoses, which has other manifestations such as the café au lait macules, and the cysts of neuro fibromatoses are more soft
Solar comedones (senile comedones). These are not uncommon in elderly people, especially in the periorbital areas. Most patients have had high exposure to UV radiation and the solar damage to the supporting dermis allows the pilo sebaceous duct to become more easily distended .
Fig.394b. Solar acne This uncommon form of acne develops in patients who wash many times daily, hoping to moderate their existing lesion. Certain bacteriostatic soaps contain weak acnegenic compounds, such as hexachlorophene which may lead to pustular and papular lesions .
The manifestations are erythema of the face usually has the appearance of butterfly where papules and papules are embedded in the erythematous patches of the face.
Fig. 397b. Acne rosacea
Drugs: such as Tetracycline, Minocycline, Doxycycline and corticosteroids. Topical corticosteroids especially when occluded may cause acniform eruption. Iodides and bromides in vitamins and mineral supplements . Other drugs such as isonicotine hydrazine (INH), ACTH, Chloral hydrates and pro-banthin can cause acniform eruption. Chemicals: Chloracne, which is due to excess chlorination of swimming pool. Chloronaphthalines, cutting oils, crude coal tar, petrol and its derivatives may cause acniform eruption.
Adolescent patients lying in bed for a long time, as in the orthopedic ward, frequently develop a flare of acne - the so-called “immobility acne.” This is probably due to a change in the environment of the skin, which may enhance bacterial colonization of the duct. The lesions characteristically occur as a result of continuous use of cosmetic creams and powders and kept for a long time without cleaning and removal. Preparations containing lanolin, petrolatum, certain vegetable oils, butylstearate, lauryl alcohol and oleic acid, are comedogenic.
Fig.401b. Cosmetic acne&contact dermatitis(Clindamycin) Grease that is applied to the scalp may cause acne.
Endocrine abnormality such as Cushing‘s disease, adrenogenital syndrome and the polycystic ovarian syndrome are associated with acne besides the other systemic manifestations.
General Considerations Dealing with acne lesion may be simple and very difficult at the same time. Too many preparations whether pharmaceutical, cosmetic, herbal, traditional, over the counter, body shop preparations and many others are available. The patients are some times confused and shift from one medication to another by himself , according to the advice of others and prescriptions from different centers. In most cases such patients will loose a lot of time , money and have their lesions usually exacerbated or accompanied by unwanted complications. The easiest way is to abide with the instructions of your physician. Playing in your lesion and spending a long time looking in your mirror and try to squeeze the pimples or pustules may lead to hazardous effect complicated by scars. Cosmetics such as powders, creams and others used as camouflage , sun blocks especially if left for a long time may lead to occlusion of the pilo sebaceous orifices leading to more and more complications. Hot humid environment should be avoided if possible. Excessive washing of the affected areas may do harmful effects, especially if certain detergents are used. Facial cleaning , peeling and others should be done by professionals and not by hairdressers, coiffeurs and inexperienced technicians. Neonatal, juvenile acne and mild types usually need no medications and if this is indicated gentle washing and mild topical preparation can be used. Regulation of sleep, stress and other negative triggering factors, should be avoided. Irritating diet if proved to have exacerbating factors should be avoided. Direct exposure to sunlight may have a good beneficial effect on acne lesion. Active Treatment Topical medications Washing the area once or twice daily with mild anti seborhea soap (Acne-aid, Neutrogena soap). Some lesions may be irritated especially young age and those with sensitive skin. Mild soaps with pH balanced such as (Seba med or Numis med soap) can be used. Erythrocin lotion (Eryderm), Clindamycin lotions (Dalacin lotion) are antibacterial . These are usually effective in pustular acne. Benzyl peroxide is effective medication .This can be applied for long standing lesions and care should be taken because of the possibility of irritation. Retinoic acid preparations such as (Retin A gel or cream, Eudyna gel). These preparations may be effective in clearing acne lesions but they may cause severe irritation if were not used properly. We begin usually with the gel form at night because it has low concentration(Retin A gel, Eudyna gel). The patient is instructed not to be exposed to direct sun light after application of such medications . The area is simply washed with water or mild soap before application of the Retin A gel. Retinoic acid preparations are rarely needed in the juvenile acne and are reserved for older age groups. Systemic Medications Different systemic medications, which are used in the adults, are not indicated for children. Eerythrocin suspension may be used for juvenile acne. Juvenile types: If the lesions are extensive , Erythrocin suspension can be used . Adult acne: Different systemic medications are used in acne affecting adults. The type of medication depends on the severity of the lesion , age and sex. The cause of acne should be discussed and the potential success of therapy be highlighted. Patient instruction leaflets are helpful. Mild acne requires only topical therapy. Patients with moderate or severe acne need both oral and topical therapy besides other lines of medical and cosmetic procedures. Oral antibiotics must be given for 6 months but topical therapy will be required throughout the duration of the disorder. These medications include the following: Tetracycline: Tetracyclines are given for a long time .Usually 250mg. is given four times daily for 10 days and the dose is reduced to twice daily for 20 days. A single daily dose may be given for 1-6 months. Tetracycline and erythromycin are bacteriostatic, especially in larger doses. In smaller doses (500mg per day or less) they do not reduce the number of organisms but they affect their function . Tetracyclines decrease the split of fats to fatty acids and triglycerides which play an important role in the inflammatory manifestations of acne. The antibiotics can also inhibit various enzyme activities and affect chemotaxis and lymphocyte functions. Care should be taken for the side effects of tetracycline. Erythromycin :This is an effective medication especially in young age and the childbearing age in females. The major disadvantage of tetracycline (and less so of erythromycin) is the need to take the tablet with water (not milk) half an hour before food: otherwise there is reduced absorption. Zithromax is an effective medication but it is more expensive than erythromycin. Doxycycline and minocycline Doxycycline (100mg/day) and minocycline (100mg/day) are effective medications but they are more expensive. We found that Doxycycline tablets are accepted well by patients, more effective than Minocycline and has fewer side effects. The dose is 100mg twice daily for ten days . The dose is reduced to 100mg daily for twenty days and 100mg every other day for three months or for a longer period depending on the lesions response. Doxycycline tablets are preferred than the capsule due to its less gastro-intestinal irritation. Oral therapy should be given for a minimum of 6 months in combination with topical therapy. Trimethoprim (400-600 mg/day), which is equally effective, can be reserved as a third-line antibiotic. Clindamycin: these are helpful because of its lipid solubility and should not be used routinely because of the possible risk of pseudomembranous colitis. Treatment of resistant adult acne lesions Change the antibiotic to Trimethoprim Prednisone 2.5 mg in the morning and 5 mg at the bed time to suppress renal androgens may help severe cases not responding to the usual lines of treatment. Suppression of adrenal androgens lead to decrease in the sebum secretions. Oral
Contraceptives Anti androgens such as Diane may be effective in controlling severe acne lesions in young girls. Cyproterone acetate (CPA) (2 mg) combined with 50-microgram ethinyl oestradiol Dianette (35 micro g. ethinyl estradiol and 2 mg CPA) appears to be of value in women with acne resistant to other therapies. Oral spironolactone 100-200 mg for 6 months, is of considerable benefit in old females. In males 25 mg CPA has been used with success . Isotretinoin is more effective than Diane for acne patients. For the patient with intractable moderate or severe acne, or if anti-androgens are unavailable, isotretinoin is the treatment of choice. Isotretinoin was restricted to adult patients with severe nodulocystic acne. Patients with less severe but scarring acne who are not responding to the traditional therapies may be given oral isotretinoin as a safe and effective treatment for severe nodulocystic acne unresponsive to conventional therapy. The usual procautions,side effects amd contra-indications should be always taken into consideration before prescribing isotretinoin to adult patients. Isotretinoin produces a striking benefit and is superior both to conventional treatment and anti-androgens. Isotretinoin is teratogenic and it is of prime importance that females using the drug should be under adequate contraception. The precautions and contra-indications of these drugs especially in adult females should be strictly considered. Fetal abnormalities and other complications may occur with these medication. Warning to the patient that pregnancy should be at least after one or two months after stopping the drug. Pregnancy test should be negative before using the medication and to be on the safe side it is advised that medication can be started on the second day of the next period. Recommended doses and duration of treatment varies . The recommended dose of isotretinoin is 0.5 -1 .0 mg/kg for younger patients and for a period of four months. Isotretinoin influences all the major factors involved in acne, in doses of 0.5-2.0mg/kg . Action of Isotretinoin
Treatment of Post Acne Scars Peeling by fruit acids such as Glycolic acid. These preparations are available in different concentrations of 10%-70%.Low concentration of 10% can be used by the patient according to the instruction of the attending physician. Peeling can give very good results for superficial scars and superficial wrinkles .
|




























| Contents | << Previous Chapter | Next Chapter >> | Search |